Mitigating Pediatric Patient Misidentification
Center for Social Design / Baltimore, Md. / September 2017
with the Johns Hopkins Armstrong Institute
Collaborating with the Johns Hopkins Armstrong Institute, the Social Design graduate candidates took a week-long dive into patient safety in Johns Hopkins Hospital’s pediatric units.
The twelve of us (three teams of four) observed the various pediatric units, including the Neonatal Intensive Care Unit (NICU), the Pediatric Intensive Care Unit (PICU), Pediatric Emergency Room, and the Pediatric Care and Clinical Research Unit.
We had a brief information session of the issue of patient safety and what that currently looks like at Johns Hopkins and we spoke with nurses to learn about how they work best, their own experiences with patient safety and patient misidentification, and what their day-to-day looks like at the hospital.
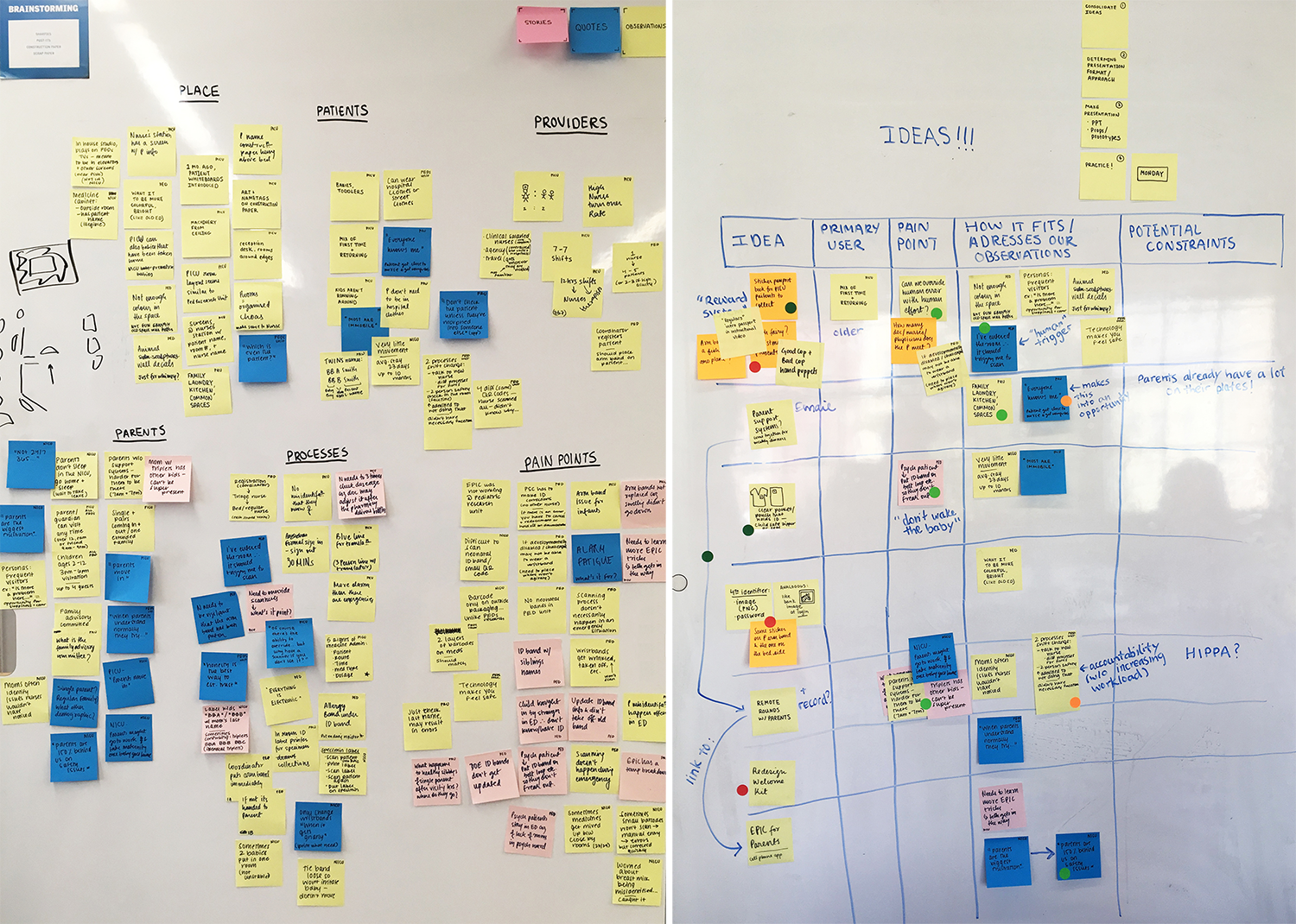
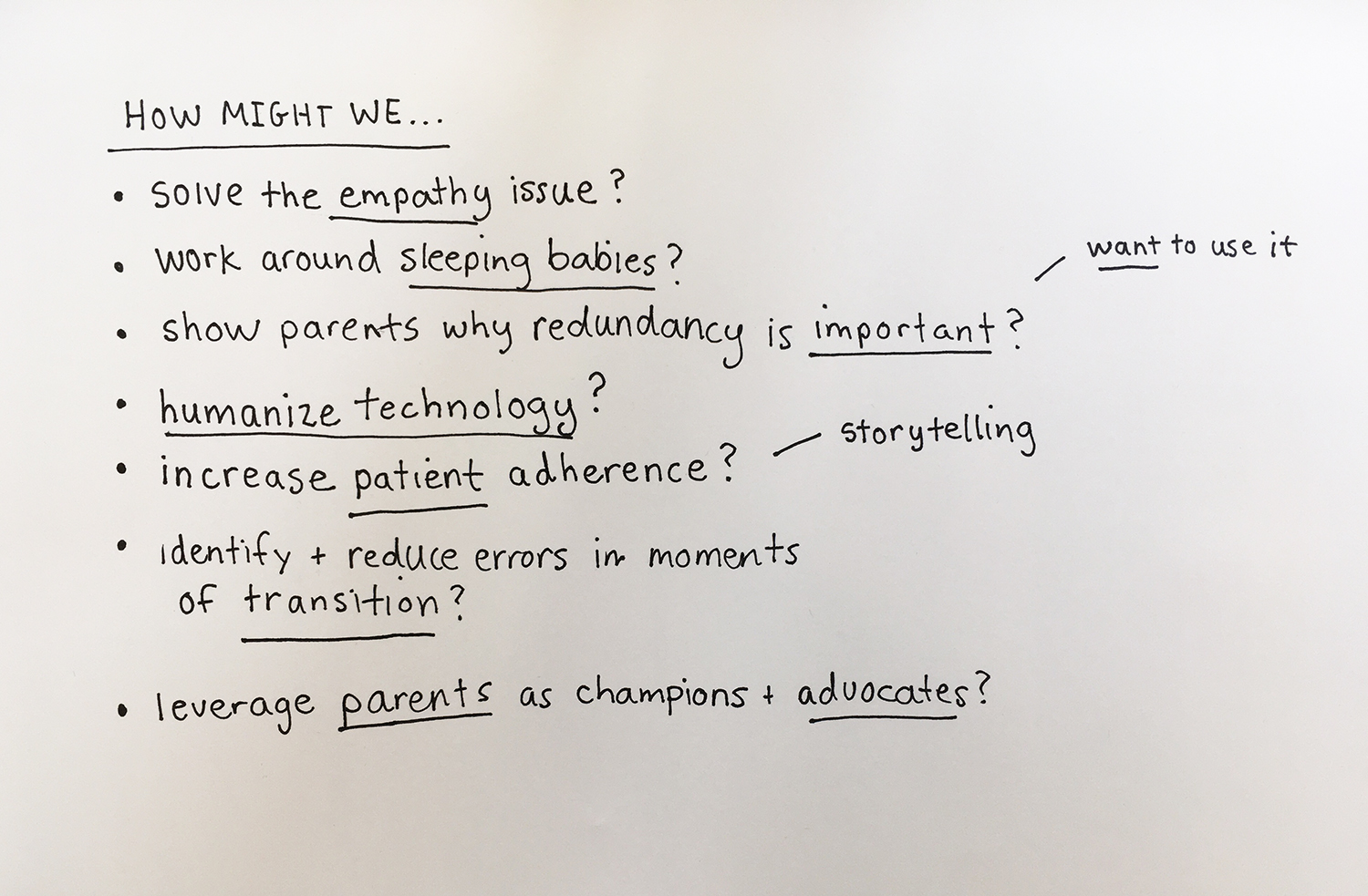
After a day of research and observation, we met with our team members to review and synthesize what we heard and saw to identify opportunities for redundancy and areas for intervention to increase patient safety.
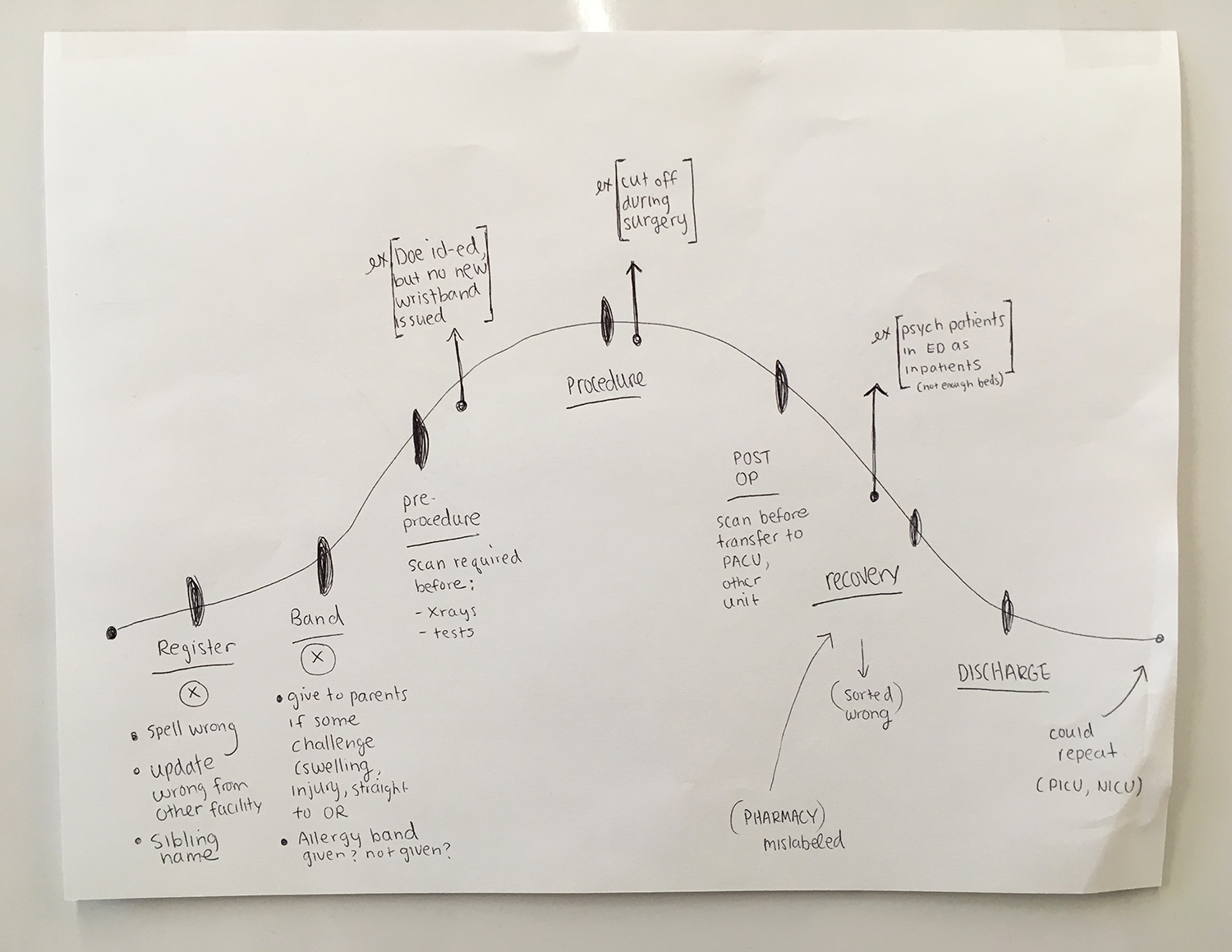
Our team created the journey map of a patient to identify their bright spots and pain points, as well as several personas to better understand the providers, patients, and guardians who were all working within this system.
In the end, our team's design concepts took different practitioner experiences into account and played on the bright spots we identified: developing playful, child-centered “nudge moments”, maximizing the parent or guardian’s ability to be a part of the child’s care team, and reconsidering traditional protocol based on how nurses work best.
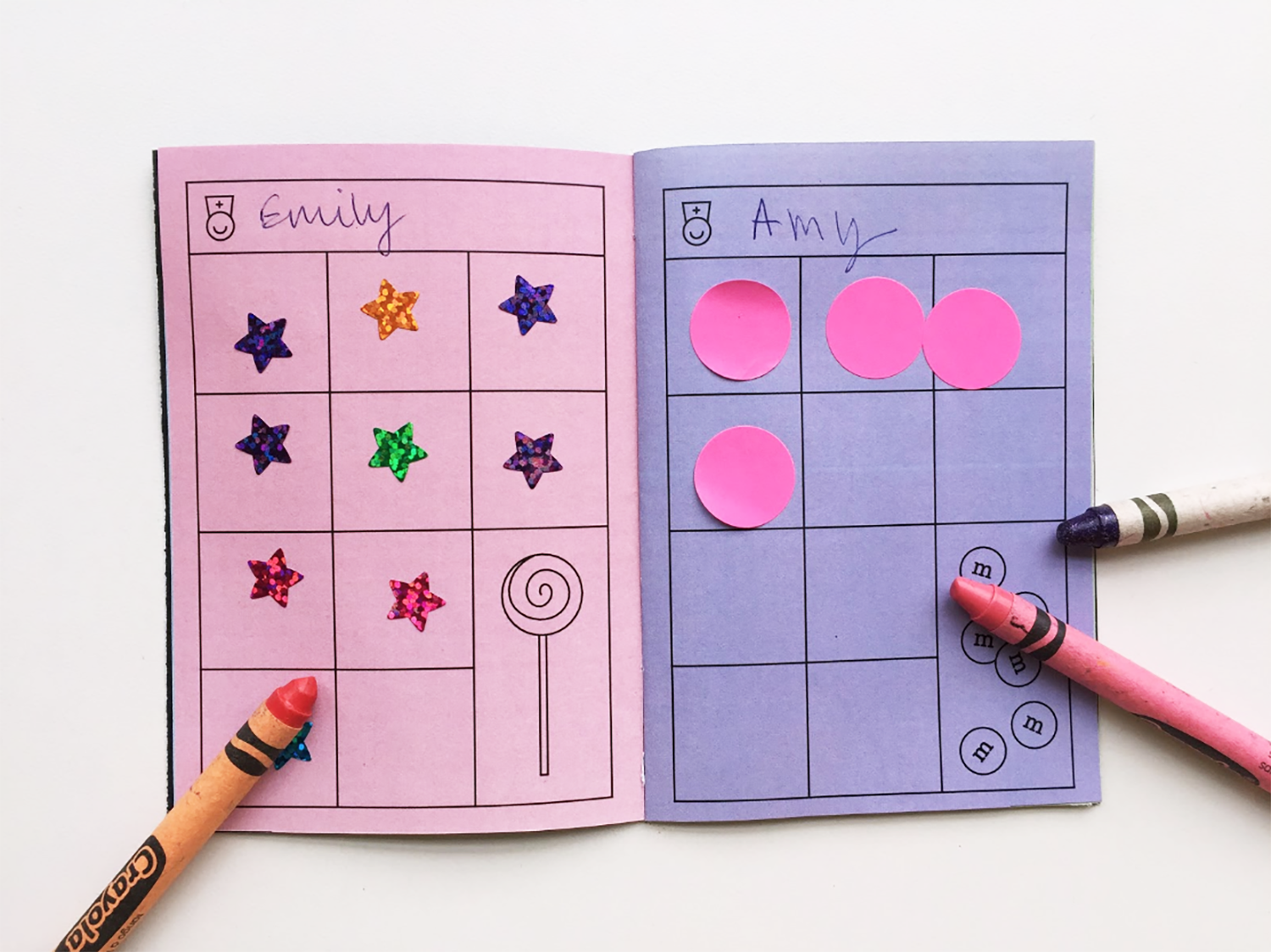
To develop playful, child-centered “nudge moments”, we had three different concepts. One was a sticker and coloring book that would incentivize the patient to make sure they are wearing their patient ID wristband and that it is being scanned each time a nurse is entering their room. This could also be a tool to help patients to remember the nurses’ names, express themselves creatively, and give them a sense of responsibility.
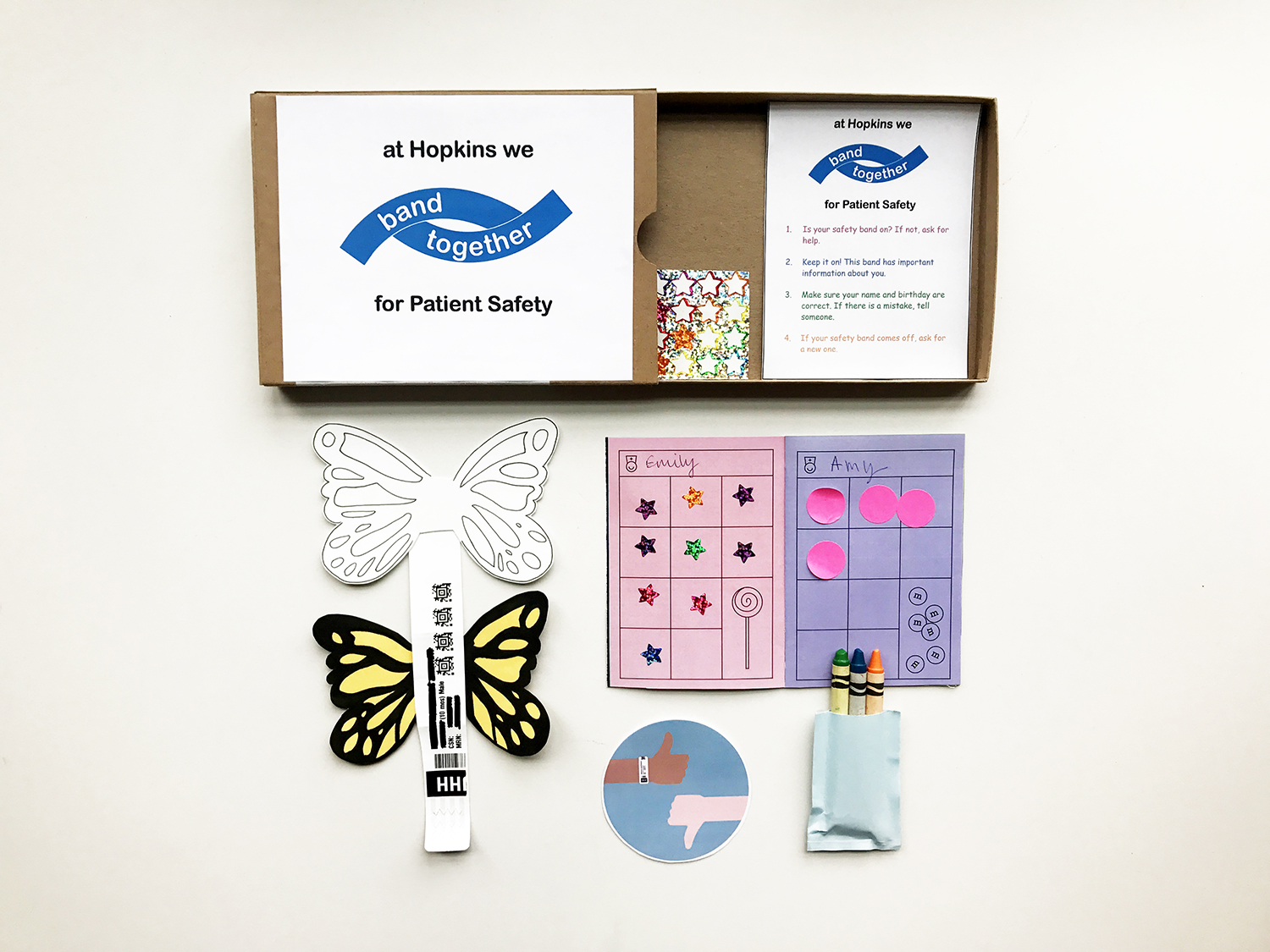
The second idea was to make the wristbands more fun and imaginative with simple, colorable add ons, like butterfly or bird wings, further encouraging the patient to wear their band.
The third concept was using puppets to teach patients about the importance of patient safety, as well as to cover the ID band scanners the nurses use, making them more inviting for the children.

To maximize the parent or guardian’s ability to be a part of the child’s care team, we came up with the concept of an interactive, online portal for parents and providers. With this portal, parents could check on what medications and dosages their child is receiving, do video check-ins with the nursing staff during turnovers, and make sure that even when they cannot physically be with their child in the hospital, they still feel involved in their child’s care.
To reconsider traditional protocol based on how nurses work best, we decided to rethink the design of how patients are identified. Johns Hopkins Hospital uses a thin, plastic band with the patient’s full name, medical ID number, and date of birth, that goes around the patient's wrist (or for infants, a band with an elongated tag). This band is easy for children to take off, it is difficult to access when babies are swaddled, and it is irritating to patients with developmental disabilities.
The first concept was inspired by one of the emergency room nurses - she told us about a patient with autism who could not wear the band on his wrist because it would trigger outbursts. She said “I wish I could just stick it on his back.” Rather than having a wristband, what if all hospital gowns and baby blankets were created with a child-proof pocket where the ID slip could sit - both on the gown’s back and front. That way nurses could access the ID without waking up a sleeping baby and it would not be something easily disposed of. Additionally, this would combat an issue in the Pediatric Research Unit, where patients are more mobile and are allowed to wear street clothes. If the ID is on the gown, all patients would be required to wear one; patients who have swapped beds or who are playing in the same bed would not be mixed up and would not be mistaken for visitors.
The second and third concepts were to rethink the band itself and the information presented on it. Rather than a thin, plastic band that creates waste, it could be more like a smartwatch or a fastpass at an amusement park. The band would be softer and less irritating on the skin, could have links that are color-coded to which units the patient has been in, and would be reusable. In addition, a fourth identifier would be added, such as an animal with a background color. Johns Hopkins Hospital assists thousands patients every year, many who may have the same name and/or birthday and may even have similar medical ID numbers. In a busy hospital, Robert Smith could easily be given the wrong Robert Smith’s ID band. To better combat this and make it kid-friendly, if a patient sees that their wristband does not have the green zebra, it would be way of notifying the patient to tell their provider something is wrong.

Our other cohort members created additional concepts, including a hospital-wide campaign to encourage the usage and wearing of ID bands, alternative forms of identification using advanced technology, and more. We determined that many of our ideas could be combined into a kit presented to parents and patients at check-in.
The Armstrong Institute was impressed with the amount of insight we had gained and the new concepts we created in such a brief amount of time.
You can view our team's presentation here.